Let’s be honest. You are reading this because you are exhausted. Not the “I need a coffee” exhaustion. The bone-deep, soul-tired exhaustion where you forget words, snap at your partner for breathing too loud, and cry in the grocery store parking lot for no reason.
You climb into bed with optimism—silk pillowcase, white noise machine, lights dimmed just right. You start to drift… and then, boom. 2:47 AM. You are drenched. Your heart pounds like you just ran a sprint. You throw off the covers, but then you freeze. You lie there, staring at the ceiling, replaying every mistake from 1998.
By 5:00 AM, you finally fall back asleep. The alarm rings at 6:15 AM. You feel like a zombie.
This is not a personal failure. This is a biological storm.
Nearly 40% to 60% of perimenopausal and postmenopausal women report significant sleep disruption. For some, it lasts 1–2 years. For others, it stretches a decade. But here is the truth that most doctors don’t tell you: You do not have to suffer through it.
In this complete guide, we will leave no stone unturned. We will cover the science, the solutions, the myths, and the emotional reality of menopause sleep problems. By the end, you will have a personalized roadmap to reclaim your rest.
The Hormonal Triad: Estrogen, Progesterone, and Testosterone
To understand menopause sleep problems, you must understand the three hormones that run the show.
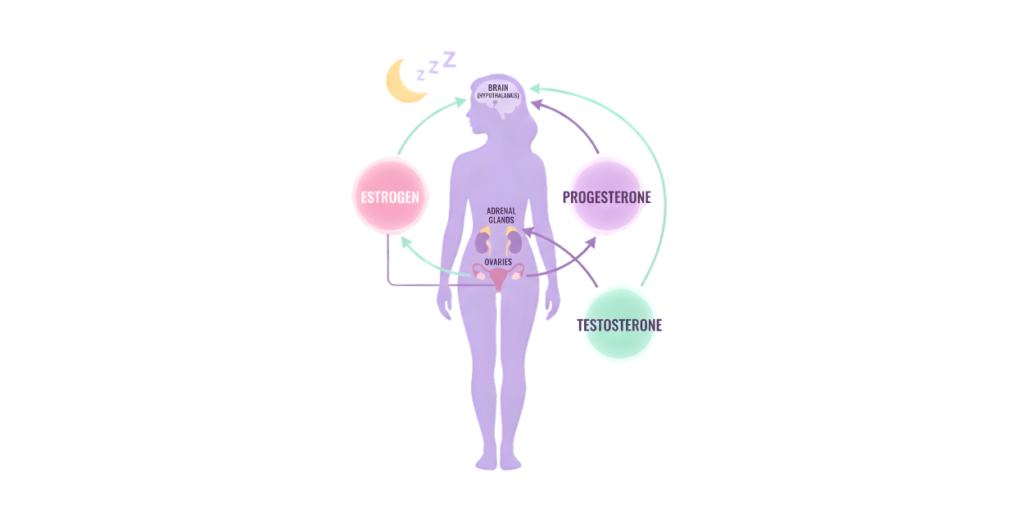
Progesterone – The Natural Sedative
Progesterone is your brain’s Valium. It binds to GABA receptors (the same ones targeted by anti-anxiety medications). It lowers body temperature, reduces neuronal firing, and induces a sense of calm.
- What happens in perimenopause: Progesterone levels drop first and fastest. You lose that nightly “sleep switch.”
- Result: Difficulty falling asleep, light fragmented sleep, and increased anxiety.
Estrogen – The Thermostat Regulator
Estrogen controls your body’s ability to regulate heat. It also helps maintain serotonin and norepinephrine levels—neurotransmitters that govern mood and sleep-wake cycles.
- What happens: Fluctuating and then declining estrogen confuses the hypothalamus (your internal thermostat). It thinks you are overheating when you are not.
- Result: Hot flashes, night sweats, and 3 AM panic attacks.
Testosterone – The Energy Modulator
We often forget testosterone, but it matters. In women, testosterone supports muscle tone, libido, and energy. Low testosterone can contribute to fatigue during the day and restless legs at night.
Data Point: A 2019 study in Menopause journal found that women with higher testosterone levels reported fewer nighttime awakenings, though the relationship is complex.
The Domino Effect
When these three hormones decline, your adrenal glands try to compensate by producing more cortisol (stress hormone). High cortisol at night is the enemy of deep sleep. You feel “tired but wired”—exhausted yet unable to shut off your racing mind.
Why Night Sweats Destroy Deep Sleep (Night Sweats Insomnia)
Let’s zoom in on the most disruptive symptom: night sweats insomnia.
The Physiology of a Hot Flash
A hot flash is not actually a rise in core body temperature. It is a miscommunication. The hypothalamus mistakenly believes you are hyperthermic. It sends a flood of chemicals (including neurokinin B and calcitonin gene-related peptide) to dilate your blood vessels and release heat.
Your skin temperature shoots up by 2–4°F in seconds. Your heart rate increases by 10–15 beats per minute. You sweat profusely.
Then, once the flash ends, your body temperature plummets, leaving you cold and clammy.
The Sleep Fragmentation Problem
Even if you don’t fully wake up, your brain leaves deep sleep (slow-wave sleep) and enters light sleep or wakefulness. Each hot flash can reduce restorative sleep by 20–30 minutes.
- One night: 4 hot flashes → loss of 1.5 to 2 hours of deep sleep.
- One week: 28 hot flashes → chronic sleep debt equivalent to pulling an all-nighter every 4 days.
The Vicious Cycle
Poor sleep increases cortisol. Cortisol worsens hot flash frequency. More hot flashes cause worse sleep. This cycle can feel unbreakable—but it is breakable, as we will show in the solutions section.
Secondary Sleep Disruptors (Anxiety, Apnea, RLS)
Hot flashes get all the attention, but menopause invites three other troublemakers into your bedroom.
Nocturnal Anxiety and Racing Thoughts
Have you ever woken up at 3 AM with a sudden, irrational fear that you forgot to pay a bill or that your child is in danger? That is nocturnal anxiety.
- Why it happens: Low estrogen reduces serotonin availability. Serotonin is converted to melatonin at night. Without enough, your brain stays in a hypervigilant state.
- The 3 AM phenomenon: Cortisol naturally rises in the early morning to help you wake up. But in menopausal women, that rise can be exaggerated, triggering panic.
Menopause-Related Sleep Apnea
Sleep apnea is not just for overweight men. After menopause, a woman’s risk equals a man’s.
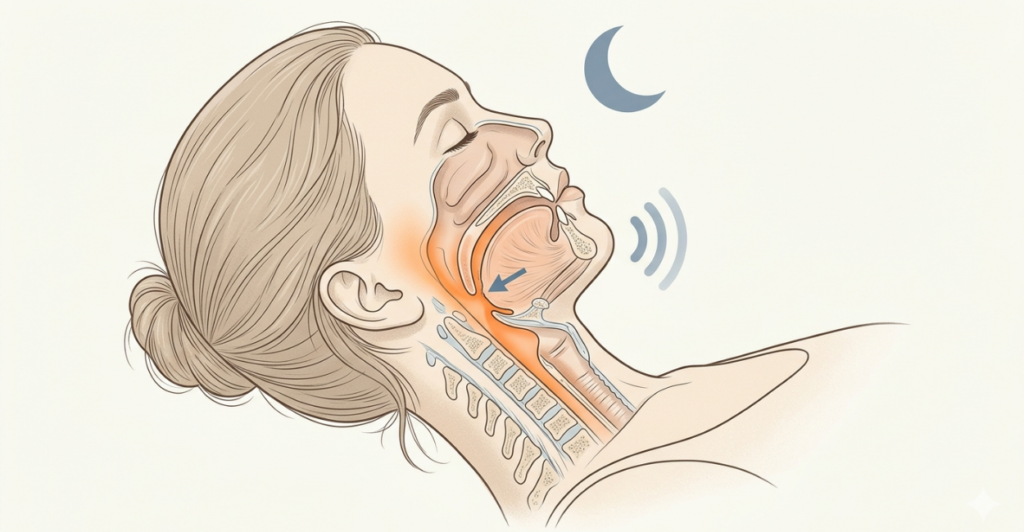
- The stat: Pre-menopause: 0.5% of women. Post-menopause: 9-15% of women (source: American Journal of Respiratory and Critical Care Medicine).
- Why: Loss of estrogen and progesterone leads to reduced muscle tone in the throat. Weight gain (common in menopause) adds mechanical pressure.
- Signs: Loud snoring, gasping/choking awakenings, morning headaches, dry mouth.
Restless Legs Syndrome (RLS)
That creepy-crawly, pulling sensation in your calves when you try to relax? That is RLS. It is twice as common in perimenopausal women as in younger women.
- Why: Iron deficiency (from heavy periods) and dopamine dysregulation. Estrogen may also play a role.
- The kicker: RLS is a movement disorder. The only relief is moving your legs, which obviously prevents sleep.
The Long-Term Health Risks of Menopause Insomnia
This is not just about feeling tired. Chronic sleep disruption during menopause has serious consequences.
| Health Area | Risk Increase | Mechanism |
|---|---|---|
| Cardiovascular disease | 45% higher risk | Inflammation, blood pressure spikes |
| Type 2 diabetes | 55% higher risk | Insulin resistance from cortisol |
| Depression | 3x higher risk | Serotonin depletion + sleep loss |
| Cognitive decline | 30% faster | Amyloid beta clearance reduced |
| Falls/fractures | 2x risk | Fatigue impairs balance |
Source: Sleep Medicine Reviews, 2022 meta-analysis of 23 studies.
The bottom line: Treating menopause sleep problems is not vanity. It is preventive healthcare.
15 Science-Backed Solutions for Menopause Sleep Problems
Here is the heart of the guide. These are actionable, evidence-based strategies. Try 2–3 at a time, not all at once.
1. Cooling Environment Hacks
Your bedroom should be a cave—cool, dark, quiet.
- Thermostat: Set to 60–67°F (15–19°C). If your partner complains, get a dual-zone cooling mattress pad.
- Fan placement: Point a fan at your torso, not your face. Evaporative cooling works best on skin.
- Freeze your pillowcase: Put a cotton pillowcase in a ziploc bag in the freezer for 2 hours before bed. Swap it out at 3 AM if needed.

2. Nutrition & Timing Strategies
- The 3-hour rule: Finish dinner 3 hours before bed. Digestion creates metabolic heat.
- Alcohol: Zero alcohol 4 hours before bed. Alcohol dilates blood vessels (triggering flashes) and fragments REM sleep.
- Spicy foods: Avoid capsaicin (chili, curry) at dinner. It raises core temperature.
- Soy isoflavones: 50-100mg of soy isoflavones daily (from tofu, edamame, or supplements) reduced hot flashes by 20% in a 2021 Nutrients study.
- Evening snack idea: 1/2 banana + 1 tablespoon almond butter. Provides magnesium, potassium, and tryptophan.
3. Cognitive Behavioral Therapy for Insomnia (CBT-I)
CBT-I is the gold standard non-pharmacological treatment. It has a success rate of 70-80% for chronic insomnia.
- Sleep restriction: Limit time in bed to actual sleep time (e.g., 6 hours). This builds sleep drive.
- Stimulus control: Bed is only for sleep and sex. No phone, no TV, no worrying. If awake >20 minutes, get up.
- Cognitive restructuring: Replace “I’ll never sleep again” with “My body is having a hard time tonight, and that is okay.”
Expert Quote: Dr. Michael Grandner, director of the Sleep and Health Research Program at the University of Arizona: “CBT-I is as effective as sleeping pills in the short term and more effective in the long term, with zero side effects.”
4. Supplements That Work (With Caveats)
Always consult your doctor before starting supplements.
| Supplement | Dose | Evidence Level | Best for |
|---|---|---|---|
| Magnesium Glycinate | 200-400mg | Strong | Calming nerves, reducing RLS |
| Black Cohosh | 40-80mg/day | Moderate | Reducing hot flashes (results vary) |
| Valerian Root | 300-600mg | Weak-moderate | Falling asleep (not staying asleep) |
| L-Theanine | 100-200mg | Moderate | Nighttime anxiety |
| Melatonin | 0.5-3mg (low dose) | Strong for circadian issues | Falling asleep early (not night waking) |

Warning on black cohosh: Rare cases of liver toxicity. Do not take if you have liver disease. Stop if you notice jaundice.
5. Hormone Replacement Therapy (HRT)
For moderate-to-severe hot flashes causing sleep disruption, HRT is the most effective intervention.
- How it works: Systemic estrogen (pill, patch, gel) stabilizes the hypothalamus. Most women see 70-90% reduction in hot flashes within 4 weeks.
- The risk profile: For women under 60 or within 10 years of menopause, benefits (sleep, bone health, quality of life) outweigh risks. The absolute risk of breast cancer from estrogen-only HRT is very low (less than 1 in 1,000 per year).
- Progesterone: If you have a uterus, you must take progesterone with estrogen to prevent uterine cancer. Progesterone also helps sleep directly.
- What to ask your doctor: “Based on my personal and family history, is the timing right for HRT?”
6. Non-Hormonal Prescription Options
If HRT is not right for you, several non-hormonal drugs are FDA-approved for hot flashes.
- Gabapentin: Originally for seizures/nerve pain. Low dose (300-900mg at night) reduces hot flashes by 45% and improves sleep continuity.
- Venlafaxine (Effexor) / Paroxetine (Brisdelle): Low-dose SSRIs/SNRIs. Reduce hot flashes by 50-60%. Brisdelle is specifically FDA-approved for hot flashes.
- Oxybutynin: An overactive bladder medication that also reduces sweating. Newer studies show 75% reduction in hot flashes.
7. Mind-Body Practices
- Box breathing before bed: Inhale 4 sec, hold 4, exhale 4, hold 4. Repeat 10 times. Lowers heart rate variability and cortisol.
- Yoga Nidra (non-sleep deep rest): A guided meditation that puts you in a state between wake and sleep. Available free on YouTube. Even 20 minutes of Yoga Nidra can restore energy equivalent to 2 hours of sleep.
- Progressive muscle relaxation: Tense each muscle group for 5 seconds, then release. Start at toes, end at face.
8. Exercise Timing Adjustments
Exercise is great for sleep, but timing matters.
- Morning (6-9 AM): Best for setting circadian rhythm. Bright light exposure + movement.
- Afternoon (1-4 PM): Safe. Body temperature naturally rises then falls.
- Evening (after 7 PM): Avoid high-intensity interval training or heavy lifting. Raises core temperature for 4-6 hours. Instead, do gentle stretching or a slow walk.
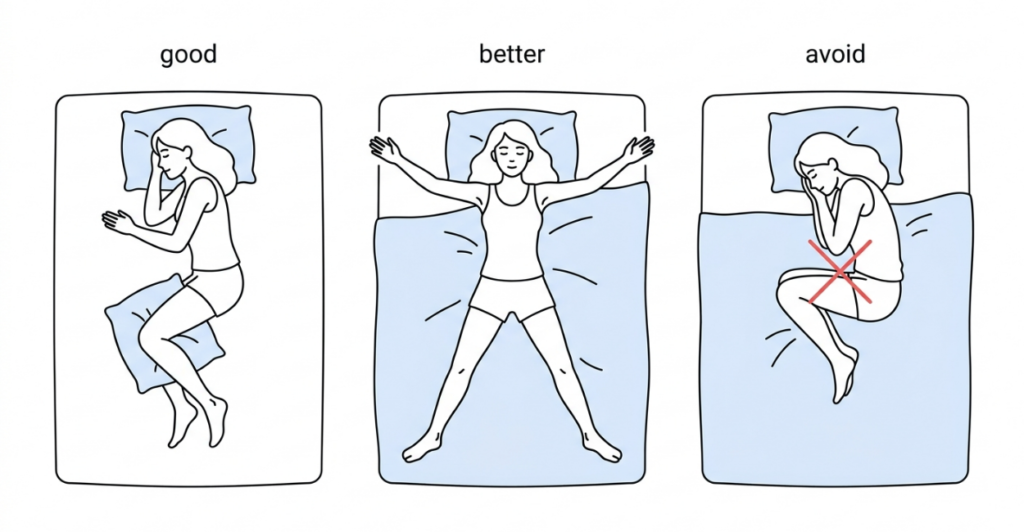
9. Sleep Position Modifications
- Side sleeping (preferably left side) reduces pressure on the vena cava and improves circulation, which can reduce hot flash intensity.
- The “starfish” position (on back with arms and legs spread) maximizes skin exposure to cool air. Use a body pillow under knees to prevent back strain.
- Avoid fetal position (curled tightly) – traps heat.
10. Bedding and Pajama Choices
- Materials to avoid: Polyester, flannel, heavy cotton flannel, memory foam (retains heat).
- Materials to buy: Bamboo viscose, Tencel (lyocell), merino wool (lightweight), linen.
- Pajama hack: Wear a thin bamboo top and no bottoms, or a cooling sleep shirt only. Less fabric = less heat trapping.
- Mattress toppers: Look for “gel-infused memory foam” or “phase-change material” (PCM). PCM absorbs heat when you are hot and releases it when you cool down.
11. Light Management
Light suppresses melatonin. Your bedroom should be a blackout cave.
- Blackout curtains: Not just dark—truly opaque. Use curtain clips to seal edges.
- Red nightlights: If you need a light to get to the bathroom, use a red bulb (red light has the least melatonin suppression).
- Blue light blockers: Wear blue-blocking glasses 2 hours before bed. They cost $15-30 on Amazon.
12. Noise Control
Menopause makes you a lighter sleeper. Protect your sleep architecture.
- White noise machine: Set to a low, continuous sound (rain, fan, brown noise). This masks sudden noises (a car horn, your partner snoring).
- Earplugs: Soft foam or silicone moldable earplugs. If you worry about not hearing your alarm, use a vibrating alarm on your smartwatch.
13. Hydration Strategy
Night sweats dehydrate you. Dehydration thickens blood, raises heart rate, and makes you feel worse.
- During the day: Drink 2-3 liters of water. Add a pinch of sea salt and a squeeze of lemon (electrolytes).
- Before bed: Stop fluids 90 minutes before sleep to prevent bathroom trips. But keep a small glass of water on your nightstand for when you wake up sweaty.
14. Stress Journaling
The “3 AM worry spiral” is real. Beat it with a pen.
- How to do it: Keep a notebook and pen by your bed. Before sleep, write down everything on your mind (to-do lists, worries, random thoughts). This is called “brain dumping.”
- If you wake up anxious: Write down the specific fear. Then write, “I cannot solve this at 3 AM. I will look at it at 9 AM.” This externalizes the worry.
15. Partner Communication
Sleep deprivation can destroy relationships. Have an honest conversation.
- The “sleep divorce”: Sleeping in separate rooms is not a sign of a failing marriage. It is a sign of a smart one. Many couples thrive with separate bedrooms.
- If you share a bed: Set rules. “No cuddling after 11 PM (too hot). If I kick you, it means I’m having a flash—please don’t take it personally.”
Myth vs. Fact: Menopause Sleep Edition
| Myth | Fact |
|---|---|
| “Only women with severe hot flashes have sleep problems.” | Fact: Even without hot flashes, hormone changes directly affect sleep architecture. Many women have insomnia without any sweating. |
| “Drinking warm milk is an old wives’ tale.” | Fact: Milk contains tryptophan, but the real benefit is the ritual and the calcium. Calcium helps regulate muscle contractions (good for RLS). |
| “If you just lose weight, the sleep problems will stop.” | Fact: Weight loss helps sleep apnea, but thin women also have severe menopause insomnia. Hormones are the primary driver. |
| “Melatonin is safe in high doses.” | Fact: High doses (10mg+) can cause vivid nightmares, morning grogginess, and actually disrupt circadian rhythms. Lower is better (0.5-3mg). |
| “HRT causes cancer, so never take it.” | Fact: For healthy women under 60, the benefits often outweigh the risks. The WHI study that caused fear was flawed (older women, specific hormone type). Talk to a menopause specialist. |
Common Mistakes That Worsen Night Sweats
- Using a weighted blanket: Great for anxiety, terrible for night sweats. The weight traps heat and reduces air circulation.
- Wearing socks to bed: Feet are major heat exchangers. Wear socks to fall asleep (warms feet, dilates vessels), then remove them after you drift off.
- Taking hot showers right before bed: A hot shower raises core temperature. You need your core to cool down to sleep. Take a warm shower 90 minutes before bed, or a cool shower 30 minutes before.
- Eating a large protein-heavy dinner: Protein digestion generates metabolic heat. Eat your largest meal at lunch.
- Sleeping with a pet: A 98°F dog or cat next to you adds significant heat. If you must co-sleep with a pet, use a cooling mat for them.
- Using synthetic “cooling” sheets that aren’t tested: Many brands claim “cooling” but are just thin polyester. Look for verified materials: Tencel, bamboo, or linen.
Real-Life Case Study: Sarah’s Journey
Name: Sarah, 52
Occupation: High school teacher
Symptoms: 6–8 night sweats per night, waking at 2 AM and unable to return to sleep, daytime brain fog, irritable with students.
What she tried first (failed):
- Over-the-counter sleep aids (diphenhydramine) – left her groggy and didn’t stop sweats.
- Cutting caffeine – helped slightly but not enough.
- Sleeping in a cold room (thermostat at 62°F) – helped reduce intensity but still woke up.
What worked (over 6 months):
- Switched to bamboo sheets and a PCM cooling mattress topper. ($150 investment)
- Started magnesium glycinate 400mg at 8 PM.
- Went to a NAMS-certified menopause specialist. Prescribed low-dose estradiol patch (0.0375mg) and oral progesterone (100mg).
- CBT-I with a therapist – 6 sessions over 8 weeks. Learned stimulus control.
- Stopped eating after 6:30 PM.
Result after 3 months: Night sweats reduced to 1–2 per night, and she falls back asleep within 10 minutes. Sleep quality score went from 4/10 to 8/10.
“I wish I had done this two years earlier. I thought suffering was normal. It’s not.” – Sarah
When to Call the Doctor (Emergency Warning Signs)
Most menopause sleep problems are not emergencies. But these symptoms require immediate medical attention.
Call your doctor within 24 hours if:
- You wake up gasping for air or choking.
- Your partner says you stop breathing for more than 10 seconds.
- You have morning headaches every day + dry mouth (signs of severe sleep apnea).
Call 911 or go to the ER if:
- You wake up with chest pain, pressure, or tightness.
- You have sudden severe headache (“thunderclap”).
- You have vision changes or slurred speech upon waking (possible stroke or TIA).
Also see a doctor if:
- You have thoughts of harming yourself or others (depression with insomnia is a risk factor for suicide – get help immediately).
- You have heavy bleeding that soaks a pad per hour for 2+ hours.
The Emotional Toll: Menopause Rage and Fatigue
Let’s talk about the shame. You lash out at your partner for the simple act of breathing. You break down over misplaced keys. And you wonder if your sanity is slipping away.
This is not a personality flaw. This is perimenopausal rage, and it is directly linked to sleep deprivation.
The Neuroscience of Rage
When you lose deep sleep, your amygdala (emotional brain) becomes 60% more reactive. Your prefrontal cortex (rational brain) becomes less active. You literally cannot regulate your emotions as well.
The Grief of Losing Your “Old Self”
Many women mourn the person they used to be—the energetic, patient, sharp woman who could handle anything. That grief is real. Allow yourself to feel it. Then remind yourself: This is a transition, not a disappearance. You are becoming a new version of you.
Practical Coping for Partners
If you have a partner, share this section with them. Ask for:
- Grace: “When I am mean at 3 AM, it’s the hormones, not me.”
- Help: “Please take over morning school drop-off so I can sleep in one day a week.”
- Space: “If I say I need to be alone, it’s not rejection.”
7-Day Sample Sleep Recovery Plan
This is a gentle, phased approach. Do not expect perfection.
| Day | Morning (6-8 AM) | Afternoon (12-3 PM) | Evening (7-10 PM) |
|---|---|---|---|
| Mon | 10 min sunlight walk | No caffeine after 2 PM | Set thermostat to 65°F. Bamboo PJs. |
| Tue | Magnesium glycinate (start 200mg) | Hydrate 2L water | No food after 7 PM. Box breathing 5 min. |
| Wed | 20 min morning exercise | 10 min afternoon stretch | Blackout curtains installed. |
| Thu | Call doctor to discuss HRT | Buy cooling pillowcase | Bed only for sleep. Get up if awake 20 min. |
| Fri | Write down 3 wins | 20 min Yoga Nidra (YouTube) | No alcohol. Warm bath 90 min before bed. |
| Sat | Sleep in (no alarm) | Brain dump journal | Separate blankets (yours cooling, partner’s warm). |
| Sun | Review sleep log | Plan next week’s sleep goals | Gratitude list before bed. |
Frequently Asked Questions
1. Can menopause cause insomnia even without hot flashes?
Yes. Hormone changes affect neurotransmitters (GABA, serotonin) independent of temperature regulation. Many women have pure hormonal insomnia with zero sweating.
2. How long do menopause sleep problems typically last?
The average duration of moderate-to-severe sleep disruption is 4 to 10 years. However, with treatment (CBT-I, HRT, lifestyle changes), most women see major improvement within 3-6 months.
3. Is it safe to take CBD or THC for menopause insomnia?
Cannabis is not FDA-approved for this use. Anecdotally, some women find low-dose THC (2.5-5mg) helps with sleep onset, but THC reduces REM sleep and can worsen anxiety long-term. CBD (without THC) has weaker evidence. Consult your doctor, especially if you take other meds.
4. Will sleeping pills damage my brain long-term?
Chronic use of anticholinergic sleep aids (diphenhydramine, doxylamine) is linked to higher dementia risk. Benzodiazepines (Valium, Xanax) are also risky. Non-benzodiazepine “Z-drugs” (Ambien, Lunesta) have lower risk but can cause dependence and next-day impairment. CBT-I is safer.
5. Can I take HRT if I had breast cancer?
Generally, no. Estrogen can feed hormone-receptor-positive breast cancer. However, non-hormonal options (gabapentin, venlafaxine, oxybutynin) are available. Talk to your oncologist.
6. Does acupuncture work for night sweats?
A 2021 meta-analysis in BMJ Open found that acupuncture reduced hot flash frequency by 30-40% compared to sham acupuncture. Results vary. It is safe and worth trying if you prefer non-drug options.
7. Why do I wake up at exactly 3 AM every night?
Your body’s cortisol naturally rises after 2 AM to prepare for waking. In menopause, that rise is exaggerated due to low estrogen. Additionally, your body temperature reaches its lowest point around 4 AM, so the temperature swing between 2-4 AM triggers thermoregulatory hot flashes.
8. Can my thyroid cause similar symptoms?
Yes. Hyperthyroidism (overactive thyroid) causes heat intolerance, sweating, and insomnia. Hypothyroidism causes fatigue. Ask your doctor for a full thyroid panel (TSH, Free T3, Free T4) to rule it out.
9. Will I ever have deep sleep again?
Absolutely. Once you identify your primary trigger (hot flashes vs. anxiety vs. sleep apnea) and treat it, your sleep architecture can fully recover. The brain is plastic; it can rebuild deep sleep.
10. Should I see a sleep specialist or a gynecologist?
Start with a NAMS-certified menopause specialist (find one at menopause.org). They understand the hormonal root. If you have signs of sleep apnea (snoring, gasping), also see a sleep medicine doctor for a home sleep test.
Final Thoughts: You Will Sleep Again
I want you to take a deep breath. Really. Do it now.
You have been through a lot. Your body is doing something extraordinary—it is transitioning from one phase of life to another. That transition comes with turbulence. But turbulence is not a crash. It is just a rough patch of air.
You now have a toolkit: cooling sheets, CBT-I, magnesium, HRT, the know-how to spot sleep apnea. You understand that 3 AM panic isn’t a glimpse of doom—just a chemical event.
Here is your homework for tonight:
- Turn your thermostat down to 65°F.
- Put on bamboo pajamas (or just a loose cotton shirt).
- Do 5 rounds of box breathing.
- Remind yourself: I am not broken. I am in transition. And I will sleep again.
You have survived every single bad night you have ever had. You will survive this one too. And with the right strategies, you will soon thrive.
Sleep well, warrior.

Bookmark this guide. Share it with a friend who woke up drenched last night. And if you found value, leave a comment below telling us one change you will make tonight.
Disclaimer
This article is for informational purposes only and does not constitute medical advice. Menopause symptoms vary widely. Always consult a qualified healthcare provider before starting any new treatment, supplement, or medication – especially hormone therapy, which requires a thorough individual risk assessment. The citations provided are current as of 2026; medical knowledge evolves rapidly. Never disregard professional medical advice because of something you have read here.
References and Trusted Sources
- National Sleep Foundation. (2021). Menopause and Sleep.
- The Menopause Society (NAMS). (2023). Nonhormonal Management of Menopause-Associated Vasomotor Symptoms.
- Guthrie, K.A., et al. (2018). Sleep duration and insomnia in menopausal women. Menopause, 25(8), 858-864.
- American College of Obstetricians and Gynecologists. (2021). Hormone Therapy for Menopause. ACOG Practice Bulletin No. 232.
- Baker, F.C., et al. (2020). Sleep and Menopause. Sleep Medicine Clinics, 15(2), 217-229.
- Mitchell, M.D., et al. (2022). CBT-I for insomnia in perimenopausal women: a randomized controlled trial. Journal of Clinical Sleep Medicine, 18(1), 101-110.
- Shifren, J.L., & Schiff, I. (2020). Role of hormone therapy in menopause. New England Journal of Medicine, 382(5), 446-453.