Medical Disclaimer: This article is for informational purposes only and does not constitute medical advice. Menopause symptoms vary. The natural remedies described are for symptom management, not medical treatment. Always consult your healthcare provider about managing menopause symptoms, including hormone therapy or other interventions. Do not stop prescribed medications without consulting your doctor.
📞 Before you try natural remedies: If you experience severe insomnia (less than 4 hours of sleep per night, multiple nights per week) or if your sleep problems are accompanied by depression, anxiety, or thoughts of self-harm, see a doctor immediately. Natural remedies are complementary tools – not replacements for professional medical care.
“I’m so tired, but I can’t sleep.”
That’s what my friend Diane whispered to me over coffee last week. She’s 52, in perimenopause, and she’s exhausted.
She falls asleep fine. But at 2 AM, she’s wide awake. Hot flash. Sweat. Then her mind starts racing: Did I send that email? Is my daughter okay? Why can’t I fall back asleep?
By 4 AM, she’s scrolling her phone. By 6 AM, the alarm goes off. She’s been “asleep” for maybe four hours. But it feels like zero.
“I’ve tried everything,” she said. “Melatonin. Magnesium. Sleep tea. Nothing works.”
I handed her my list – the same one I’m sharing with you.

This article is for anyone who:
- Falls asleep easily but wakes up at 2 AM and can’t go back to sleep
- Lies awake for hours with a racing mind
- Has tried melatonin and magnesium without success
- Wants natural, evidence-based solutions – not sleeping pills
I’ve spent months researching the science behind menopause insomnia – from clinical trials to systematic reviews. I’ve interviewed sleep specialists and talked to women who’ve tried everything.
Here’s what actually works.
Why Menopause Causes Insomnia (It’s Not Just Hot Flashes)
Let’s be honest: most people think menopause insomnia is just about hot flashes. Wake up sweating, throw off covers, fall back asleep. Simple.
But it’s not that simple.
Menopause disrupts sleep in multiple ways:
| Cause | What Happens |
|---|---|
| Hormonal shifts | Declining estrogen and progesterone disrupt the sleep-wake cycle. Progesterone is a natural sedative; when it drops, sleep becomes lighter and more fragmented. |
| Melatonin disruption | Estrogen helps regulate melatonin secretion. When estrogen drops, your internal clock (circadian rhythm) can go off course. |
| Hot flashes & night sweats | Vasomotor symptoms can jolt you awake multiple times per night, making it hard to return to deep sleep. |
| Anxiety & racing thoughts | Menopause can worsen anxiety, creating a vicious cycle: you can’t sleep, so you worry, so you really can’t sleep. |
| Sleep apnea risk | The “tipping point” of late perimenopause can unmask obstructive sleep apnea, which is often misdiagnosed in women. |
The scale of the problem is staggering. Research shows that 50%–55% of perimenopausal women experience sleep disorders. A 2025 survey of over 26,000 women found that 90.3% reported at least some degree of sleep disturbance, with nearly half (48%) meeting criteria for clinical insomnia. Another large-scale study of Chinese women found that insomnia (50.0%) was the most commonly reported menopausal symptom – more common than fatigue or nervousness.
And the stakes are high. Persistent insomnia symptoms are associated with a 71% increased incidence of cardiovascular events, independent of hot flashes.
So yes, menopause insomnia is real. And it deserves real solutions.
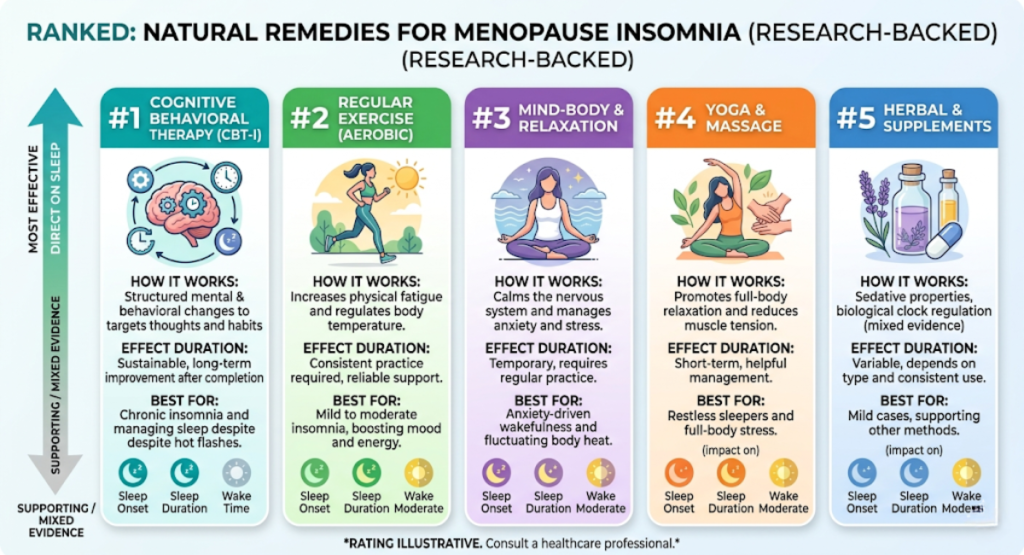
The 8 Most Effective Natural Remedies for Menopause Insomnia (Ranked by Research)
A major 2025 network meta-analysis of 44 trials (3,512 participants) ranked non‑pharmacological interventions for menopause‑related insomnia.
Here’s the ranking from most to least effective (based on effect size):
| Rank | Remedy | Effect Size (MD) | What It Means |
|---|---|---|---|
| 1 | Mindfulness | -5.61 (95% CrI: -8.70 to -2.50) | Most effective – large improvement in sleep quality |
| 2 | Relaxation techniques | -4.80 | Highly effective – reduces nighttime arousal |
| 3 | Cognitive Behavioral Therapy for Insomnia (CBT-I) | -4.20 | Proven first‑line treatment – works for chronic insomnia |
| 4 | Massage | -3.90 | Reduces muscle tension and anxiety |
| 5 | Aromatherapy | -3.50 | Effective when combined with other approaches |
| 6 | Yoga | -3.10 | Combines movement, breath, and mindfulness |
| 7 | Exercise | -2.40 | Moderate effect – best with regular practice |
| 8 | Acupuncture | -2.10 | Gentle, cumulative effect |
Source: Effectiveness of nonpharmacological interventions for menopause‑related insomnia: A systematic review and Bayesian network meta‑analysis, Maturitas, November 2025
Let’s dive into each of these – plus a few more that didn’t make the top eight but are worth knowing about.
1. Mindfulness (Most Effective)
Why it works: Mindfulness trains your brain to observe thoughts without getting caught up in them. When you wake up at 2 AM with a racing mind, mindfulness helps you let the thoughts pass – without spiraling into anxiety.
A 2025 meta‑analysis of 18 studies (1,572 participants) found that mindfulness significantly improved sleep quality in menopausal women (SMD = -0.86). A separate network meta‑analysis ranked mindfulness as the most effective non‑pharmacological intervention for menopause‑related insomnia.
What it looks like in practice:
- 8‑week Mindfulness‑Based Stress Reduction (MBSR) program – weekly 60–90 minute sessions, plus daily home practice (body scan, breathing awareness, mindful movement)
- Apps – Calm, Headspace, Insight Timer (10‑minute daily practice is enough to start)
Who it’s for: Women whose main problem is waking up with a racing mind. Also effective for anxiety and depression, which often accompany menopause insomnia.
The trade‑off: Takes practice. Results aren’t instant. But the benefits compound over time.
“Mindfulness-based therapies can be recommended as non‑pharmacologic options to manage sleep disturbances during menopause.” — Frontiers in Public Health, 2025
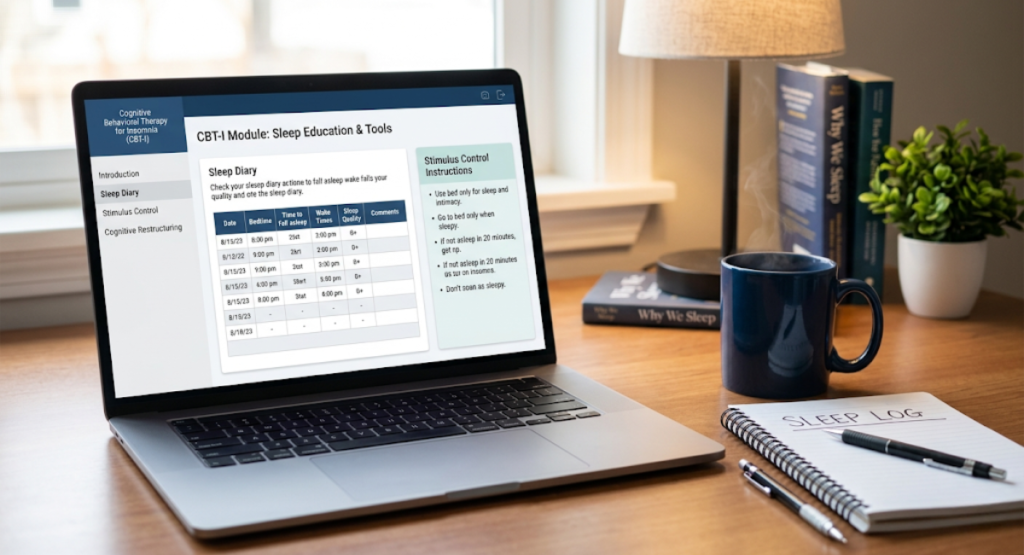
2. Cognitive Behavioral Therapy for Insomnia (CBT‑I)
Why it works: CBT‑I addresses the thoughts and behaviors that perpetuate insomnia. It’s not about “relaxing” – it’s about retraining your brain and body to associate the bed with sleep, not wakefulness.
A 2024 scoping review found that CBT‑I significantly improves sleep quality and reduces insomnia severity in menopausal women, with improvements persisting for up to six months after treatment. CBT‑I was particularly effective compared to sleep restriction therapy and sleep hygiene education alone.
What it looks like in practice:
- Stimulus control – Get out of bed if you can’t sleep (don’t lie there awake)
- Sleep restriction – Limit time in bed to actual sleep time
- Cognitive restructuring – Challenge unhelpful thoughts (“I’ll never sleep again”)
- Sleep hygiene – Consistent bedtime/wake time, no screens before bed
Delivery options: Face‑to‑face, online, or telephone‑based – all effective.
Who it’s for: Women with chronic insomnia (three or more nights per week for three months). Works regardless of baseline severity or delivery format.
The trade‑off: Requires commitment (typically 6–8 sessions). Not a quick fix. But the results last.
3. Exercise
Why it works: Exercise reduces anxiety, regulates body temperature, and increases slow‑wave (deep) sleep.
A 2024 meta‑analysis of 16 studies found that low‑ and moderate‑intensity aerobic exercise had a moderate effect on sleep disorders in menopausal women (SMD = -0.52, P < 0.001).

The most effective dosage (based on research):
| Factor | Optimal |
|---|---|
| Frequency | 3 times per week |
| Duration per session | 70–90 minutes |
| Program length | 8–10 weeks |
| Type | Aerobic (walking, swimming, cycling) |
| Mode | Individual exercise (but group improves adherence) |
Source: BMC Women‘s Health, 2024
What it looks like in practice:
- Morning: 30‑minute brisk walk (regulates circadian rhythm)
- Afternoon: Yoga or swimming (reduces evening anxiety)
- Evening: Light stretching only (intense evening exercise can delay sleep)
Who it’s for: Women who are sedentary or have mild‑to‑moderate sleep issues. Also improves mood, bone density, and cardiovascular health – all relevant during menopause.
The trade‑off: Takes time. Morning exercise is better for sleep than evening exercise.
4. Mind‑Body Exercises (Yoga, Tai Chi, Qigong)
Why they work: Mind‑body exercises combine physical movement with breath awareness and meditation – addressing both the body and the anxious mind.
A 2024 meta‑analysis of 11 RCTs (1,005 participants) found that mind‑body exercise significantly improved sleep quality in perimenopausal and postmenopausal women (SMD = -0.48). It also significantly reduced anxiety and depression.
What works best: Yoga, tai chi, qigong, and Pilates all showed benefits.
What it looks like in practice:
- Restorative yoga before bed (legs‑up‑the‑wall, child’s pose)
- Tai chi in the morning (improves balance and sleep quality)
- Qigong (gentle, flowing movements)
Who it’s for: Women who enjoy movement but find high‑intensity exercise unappealing. Excellent for those with anxiety or joint pain.
The trade‑off: May not be enough for severe insomnia alone – works best combined with CBT‑I or mindfulness.
5. Aromatherapy (Especially Lavender)
Why it works: Inhaling lavender oil activates the parasympathetic nervous system, lowering heart rate and blood pressure.
A 2025 network meta‑analysis found that aromatherapy significantly improved sleep quality in menopausal women. A 2026 randomized controlled trial found that Cognitive Behavioral Group Therapy combined with lavender aromatherapy significantly improved sleep quality in post‑menopausal women.
What it looks like in practice:
- Lavender essential oil in a diffuser – run for 30 minutes before bed
- Lavender pillow spray – spritz on pillowcase (avoid eyes)
- Diluted lavender oil on wrists – mix with carrier oil (test skin first)
Who it’s for: Women who find scent soothing. Works well as a complementary therapy alongside CBT‑I or mindfulness.
The trade‑off: Not enough as a standalone treatment for severe insomnia. Some people are sensitive to strong scents.
6. Acupuncture
Why it works: Acupuncture may regulate neurotransmitters (GABA, serotonin) and reduce inflammation, both of which affect sleep.
A 2024 meta‑analysis of 16 RCTs (1,112 participants) found that acupuncture significantly improved sleep quality compared to sham‑acupuncture (PSQI MD -3.94) and medication (PSQI MD -2.62). Objective measures showed that acupuncture improved sleep efficiency and total sleep time.
Safety: Adverse events were infrequent and generally mild. Acupuncture had a lower risk of adverse events compared to medication (RR 0.05).
What it looks like in practice:
- 10 sessions over 4–6 weeks (typical course)
- Maintenance sessions every 2–4 weeks as needed
Who it’s for: Women who prefer non‑pharmacological, hands‑on treatments. Works best for mild‑to‑moderate insomnia.
The trade‑off: Requires finding a licensed, experienced acupuncturist. May not be covered by insurance. Evidence is low‑to‑moderate quality.
7. Relaxation Techniques (Progressive Muscle Relaxation, Deep Breathing)
Why it works: These techniques reduce sympathetic nervous system activity (the “fight or flight” response), lowering heart rate and blood pressure.
The network meta‑analysis ranked relaxation techniques as the second most effective intervention for menopause‑related insomnia.
What it looks like in practice:
- Progressive Muscle Relaxation (PMR) – Tense and release each muscle group from toes to head (10–15 minutes)
- 4‑7‑8 breathing – Inhale for 4 seconds, hold for 7, exhale for 8 (repeat 5–8 times)
- Body scan – Mentally scan your body from head to toe, noticing sensations without judgment
Who it’s for: Women whose insomnia is driven by physical tension or stress. Excellent for falling asleep – and for returning to sleep after a 2 AM wake‑up.
The trade‑off: Requires practice. Works best when done daily, not just during insomnia episodes.
8. Dietary and Nutritional Interventions
Why it works: Certain foods contain nutrients that support melatonin production (tryptophan) or have direct sleep‑promoting effects (magnesium, calcium, tart cherry juice).
A 2025 systematic review found that nutritional interventions may alleviate menopause‑related sleep disturbances, with studies showing that tart cherry juice and tryptophan‑rich foods can improve relevant aspects of sleep.
Sleep‑promoting nutrients:
| Nutrient | Food Sources | How It Helps |
|---|---|---|
| Tryptophan | Turkey, chicken, eggs, salmon, nuts, seeds, oats, quinoa, milk | Precursor to serotonin and melatonin |
| Magnesium | Spinach, almonds, pumpkin seeds, dark chocolate (70%+ cocoa) | Relaxes muscles, reduces anxiety |
| Calcium | Dairy, leafy greens, fortified plant milks | Helps brain use tryptophan to make melatonin |
| Melatonin | Tart cherries, walnuts, grapes | Directly supplements sleep hormone |
What to eat (and when):
- 2–3 hours before bed: Light snack with tryptophan + complex carb (e.g., banana with almond butter, small bowl of oatmeal)
- Avoid: Large meals, spicy foods, caffeine (after 2 PM), alcohol (disrupts sleep architecture)
Who it’s for: Women who prefer food‑based solutions. Works best for mild insomnia or as part of a broader strategy.
The trade‑off: Dietary changes alone are rarely enough for moderate‑to‑severe insomnia.
Herbal & Supplemental Aids (Use with Caution)
These are not ranked as highly as behavioral interventions, but some women find them helpful. Always consult your doctor before starting supplements.
Melatonin
What the research says: A 2024 systematic review found that melatonin use in postmenopausal women was associated with some improvements in anxiety and depression compared to placebo. However, a 2024 randomized controlled trial found no significant improvement in sleep quality with 10 mg melatonin daily compared to placebo.
Dosage: 1–3 mg, 60 minutes before bed. Start low. Some studies used 2 mg sustained‑release.
The trade‑off: Results are mixed. Works for some, not for others. May cause morning grogginess.
Magnesium
What the research says: A 2010 RCT in older adults (51+ years) found that 320 mg magnesium citrate daily for 8 weeks significantly reduced PSQI scores from 10.4 to 6.6 (P < 0.0001). However, a 2022 RCT in younger women (18‑45 years) found no significant improvement in sleep quality after 10 weeks of 250 mg magnesium oxide. Another 2022 RCT in hospitalized patients found significant improvements after 5 days of 500 mg magnesium oxide (P = 0.021).
Conclusion: Results are inconsistent. Magnesium may work better in older adults or when combined with other supplements (e.g., magnesium + melatonin).
Dosage: 200–400 mg daily, preferably as magnesium glycinate or citrate (better absorption).
The trade‑off: Not a guaranteed solution. May cause digestive upset.
Valerian Root
What the research says: A randomized controlled trial in menopausal women found that valerian improves the quality of sleep in women experiencing insomnia. Two small randomized studies also reported a decrease in menopausal hot flashes with valerian compared to placebo after 4 and 8 weeks.
Dosage: 400–900 mg, 30–60 minutes before bed. One trial used 1000 mg/day (two capsules).
The trade‑off: Evidence is limited. May cause vivid dreams or morning grogginess.
Black Cohosh
What the research says: Black cohosh is primarily studied for hot flashes, not directly for insomnia. Some studies suggest it may improve sleep as a secondary benefit. One 2023 study found that black cohosh increased sleep efficiency and reduced wake‑after‑sleep onset by 15.8% compared to placebo. However, safety concerns and uncertainty about appropriate dosing mean it’s not currently recommended by many experts.
The trade‑off: Mixed evidence. Potential liver toxicity with long‑term use. Not recommended without medical supervision.
East Asian Herbal Medicine (EAHM)
What the research says: A 2024 systematic review and meta‑analysis of 70 RCTs (6,035 participants) found that EAHMs – particularly modified Suan Zao Ren Tang – significantly improved sleep quality compared to sedative‑hypnotics (PSQI MD –2.18). EAHM was also generally safer than sedative‑hypnotics, with significantly fewer adverse reactions (RR 0.15).
Examples: Suan Zao Ren Tang (Sour Jujube Decoction) is one of the most frequently used formulas.
The trade‑off: Must be prescribed by a qualified practitioner of Chinese medicine. Herbal quality and dosing vary. Evidence certainty is moderate to low.
Emerging Therapies (Promising but Early)
Bright Light Therapy
Why it works: Resets the circadian rhythm, which can become misaligned during menopause. Morning bright light advances the internal clock, helping with early‑morning awakenings.
A 2024 clinical trial at UCSD is investigating whether critically‑timed sleep + light interventions can correct circadian misalignment in perimenopausal women and improve mood and sleep within 1–2 weeks.
What it looks like in practice: Sit in front of a 10,000 lux light box for 30 minutes within 30 minutes of waking up.
Who it’s for: Women with early‑morning awakenings (3–4 AM) or delayed sleep phase (can‘t fall asleep until 1‑2 AM).
The trade‑off: Not a first‑line treatment. Still being studied for menopause specifically.
Myth vs. Fact: Menopause Insomnia Edition
Common Mistakes to Avoid
- Relying solely on supplements without addressing behavior – Melatonin won’t fix poor sleep hygiene. Start with CBT‑I or mindfulness.
- Using screens in bed – Blue light suppresses melatonin. Keep phones out of the bedroom.
- Drinking caffeine after 2 PM – Caffeine’s half‑life is 5‑6 hours. Even afternoon coffee can disrupt sleep.
- Exercising too close to bedtime – Intense evening exercise raises core body temperature and delays sleep onset.
- Expecting overnight results – Most natural remedies take 2‑4 weeks to show benefits. Be patient.
- Ignoring underlying sleep disorders – Menopause can unmask sleep apnea. If you snore, gasp, or wake up with headaches, get a sleep study.
- Not keeping a sleep diary – Tracking patterns helps identify triggers and measure progress.
Your Menopause Insomnia Action Plan (Printable Checklist)
Weeks 1‑2: Foundation
- Set a consistent wake time (even on weekends)
- Get morning sunlight within 30 minutes of waking
- No caffeine after 2 PM
- Stop eating 2‑3 hours before bed
- Start a 5‑minute wind‑down routine (deep breathing or PMR)
Then Weeks 3‑4: Add Behavioral Techniques
- Try a 10‑minute mindfulness or body scan before bed
- If you wake up at 2 AM, get out of bed after 20 minutes (read in dim light, no screens)
- Start a sleep diary (track bedtime, wake time, awakenings, caffeine/alcohol)
Finally, Week 5‑8: Optimize
- Add aerobic exercise: 3x/week, 70‑90 minutes, morning or afternoon
- Try yoga or tai chi 2‑3x/week
- Consider lavender aromatherapy (diffuser or pillow spray)
If Still Struggling After 8 Weeks:
- Consult a CBT‑I specialist (online options available)
- See your doctor to rule out sleep apnea, thyroid disorders, or depression
- Ask about prescription options (non‑hormonal or low‑dose HRT)
Real‑Life Examples: Women Who Found Relief
Margaret, 55 (post‑menopause): “I was waking up at 3 AM every night, wide awake for hours. My doctor suggested CBT‑I. I did 6 sessions online. Now I sleep 6‑7 hours straight. I never thought that was possible.”
Sarah, 49 (perimenopause): “I couldn’t afford therapy. I started with 10 minutes of mindfulness using an app. At first, nothing changed. But after 3 weeks, I noticed I was falling back asleep faster after hot flashes. It’s not perfect, but it’s better.”
Elena, 52 (on HRT): *“HRT helped my hot flashes but not my sleep. I added morning walks (3x/week) and lavender oil at night. Now I sleep through the night about 5 nights a week. That‘s a win for me.”*
Case Study: One Woman, Three Approaches
Subject: Diane, 52, perimenopause – wakes up at 2 AM, stays awake for 1‑3 hours, 6‑7 nights per week.
| Approach | Result |
|---|---|
| Melatonin (3 mg) + magnesium | No change after 4 weeks. Still waking up. |
| Sleep hygiene alone | Small improvement (waking 5‑6 nights instead of 7). |
| CBT‑I (8 weeks, online) | Waking reduced to 2‑3 nights per week. Sleeps through on good nights. |
Conclusion: Behavioral interventions (CBT‑I, mindfulness) had the biggest impact – not supplements.
🚨 When to See a Doctor (Not Just Try Natural Remedies)
If you experience any of the following, see a doctor:
- Less than 4 hours of sleep per night, most nights – This can impair immune function and increase cardiovascular risk.
- Loud snoring or gasping during sleep – Possible sleep apnea, which is common in menopause and often underdiagnosed.
- Depressed mood or thoughts of self‑harm – Menopause can worsen mood disorders. Get help immediately.
- Night sweats that soak through bedding every night – Could indicate an underlying medical condition.
- Daytime sleepiness affecting driving or work – Falls and accidents are real risks.
Persistent insomnia symptoms are associated with a 71% increased incidence of cardiovascular events. Don‘t ignore your sleep problems.
Frequently Asked Questions
What is the most effective natural remedy for menopause insomnia?
Mindfulness and CBT‑I are the most effective non‑pharmacological interventions, based on the most recent network meta‑analysis. Both have large effect sizes and lasting benefits.
How long does it take for natural remedies to work?
2‑4 weeks for noticeable improvements with behavioral interventions (CBT‑I, mindfulness, exercise). 8‑12 weeks for full benefits. Supplements may work faster (1‑2 weeks) but results are less consistent.
Can I use melatonin if I‘m on HRT?
Generally yes, but consult your doctor. Melatonin can interact with blood thinners, diabetes medications, and immunosuppressants. Start with a low dose (1‑3 mg).
Is exercise better in the morning or evening for sleep?
Morning or afternoon is best. Intense evening exercise (within 2‑3 hours of bed) can delay sleep onset. Light stretching or yoga in the evening is fine.
What’s the difference between CBT‑I and sleep hygiene?
Sleep hygiene is basic: keep a consistent schedule, avoid caffeine, make your bedroom dark and cool. CBT‑I is a structured, multi‑session therapy that addresses the thoughts and behaviors driving insomnia. CBT‑I is significantly more effective than sleep hygiene alone.
Can diet alone cure menopause insomnia?
No. Dietary changes (tart cherry juice, tryptophan‑rich foods) can help, but they are rarely enough for moderate‑to‑severe insomnia. Combine with behavioral approaches.
My Final Verdict: Where to Start
| Your Situation | Start Here |
|---|---|
| Mild insomnia (1‑2 nights/week, minimal daytime impact) | Sleep hygiene + morning exercise + lavender aromatherapy |
| Moderate insomnia (3‑4 nights/week, some daytime fatigue) | Mindfulness app (10 min/day) + progressive muscle relaxation before bed |
| Severe insomnia (5+ nights/week, significant daytime impairment) | CBT‑I (online or in‑person) + consult your doctor |
| Waking up gasping or snoring loudly | Sleep study – possible sleep apnea |
| Hot flashes are your main sleep disruptor | Cooling bedding + moisture‑wicking pajamas + HRT (talk to your doctor) |
Here’s my advice: Start with the simplest intervention – morning exercise and 10 minutes of mindfulness before bed. Give it 4 weeks. Track your sleep in a diary. If you’re not seeing improvement, add CBT‑I (online programs are affordable and effective). Save supplements for last – they’re less reliable than behavioral changes.
Your best night of sleep is not a distant memory. It’s within reach.
Ready to take control of your menopause insomnia? [Click here] to see my recommended CBT‑I apps and mindfulness tools.
Download my free PDF: “Menopause Insomnia Action Plan” – no email required.
Medical References & Trusted Sources
- CBT‑I for menopausal insomnia – Life (2024), PMC11595697.
- Mind‑body therapies for sleep disturbances – Frontiers in Public Health (2025), 10.3389/fpubh.2025.1686981.
- Nonpharmacological interventions for menopause insomnia – Maturitas (2025), 10.1016/j.maturitas.2025.108713.
- Aerobic exercise for sleep disorders in menopause – BMC Women‘s Health (2024), 10.1186/s12905-024-03477-2.
- Mind‑body exercise for menopause symptoms – Menopause (2024), 10.1097/GME.0000000000002336.
- East Asian herbal medicine for menopausal insomnia – Frontiers in Pharmacology (2024), 10.3389/fphar.2024.1414700.
- Acupuncture for perimenopausal insomnia – European Journal of Integrative Medicine (2024).
- Sleep disorders affect 50‑55% of perimenopausal women – European Journal of Endocrinology (2025), 10.1093/ejendo/lvag029.
- Prevalence of insomnia in menopausal women (50%) – China CDC Weekly (2025), 7(10):334‑340.
- Insomnia severity in menopausal women (48% clinical insomnia) – IJERPH (2025), 10.3390/ijerph22101502.
- Mindfulness‑Based Stress Reduction for menopause – ICH GCP (2026), NCT07402096.
- Bright light therapy for menopausal sleep – UCSD Clinical Trial (2024), NCT06678880.
Medical Disclaimer (repeated): This article is for informational purposes only. The natural remedies described are for symptom management, not medical treatment. Always consult your healthcare provider about managing menopause symptoms. Do not stop prescribed medications without consulting your doctor.
Last updated: April, 2026
Published: April, 2026