You drift off to sleep easily, exhausted from the day. But like clockwork, your eyes snap open at 3:00 AM. Your heart isn’t racing, but your mind is suddenly wide awake. The ceiling stares back at you for two hours until the alarm goes off.
If this scenario feels personal, you are not broken. You are not simply “bad at sleeping.” You are likely experiencing a symphony of chemical messengers playing the wrong tune. Meet the three conductors of your nightly restoration: estrogen, progesterone, and cortisol.
We often blame stress or a bad mattress for poor sleep. But for millions of people—especially women navigating menstrual cycles, pregnancy, or menopause—the root cause is invisible, internal, and hormonal. This article will pull back the curtain on how these three hormones interact with your brain’s sleep architecture. setting up a sleep routine is crucial for menopausal women different life stages and, most importantly, what you can do about it.
The Hormonal Sleep Orchestra (An Overview)
To understand insomnia, you must first understand that sleep is not a passive state. It is an active biological process involving two main systems: the circadian rhythm (your internal clock) and the homeostatic sleep drive (your need for rest). Hormones act as the messengers between these systems.
- Cortisol is the accelerator. It wakes you up.
- Progesterone is the brake pedal. It calms you down.
- Estrogen is the steering wheel. It regulates temperature and mood, keeping the ride smooth.
When one of these is out of balance, the vehicle crashes. Let’s look at each driver individually before seeing how they collide.
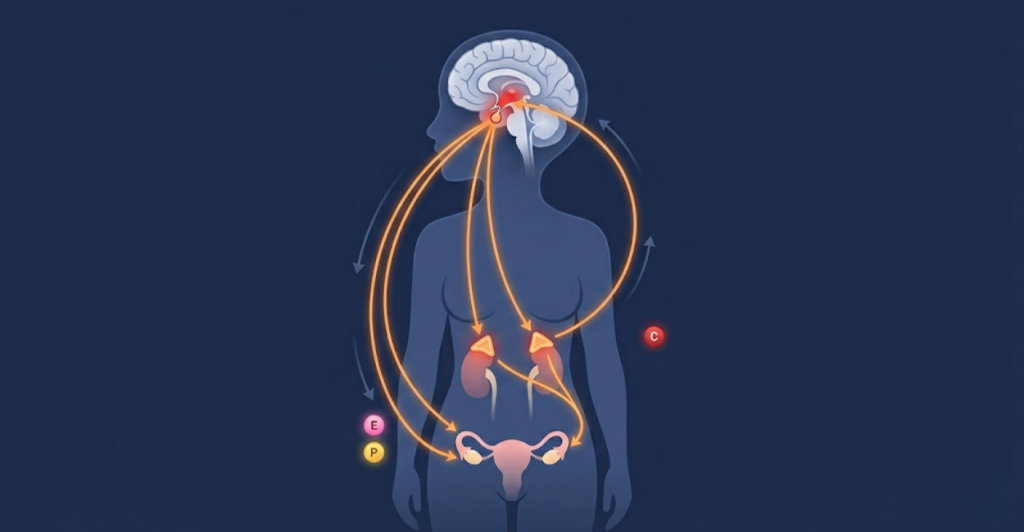
What is the HPA Axis?
The Hypothalamic-Pituitary-Adrenal (HPA) axis is the command center. Your brain detects stress or light, signals the pituitary gland, which then tells your adrenal glands to release cortisol. Simultaneously, the ovaries release estrogen and progesterone based on signals from the brain. Sleep and hormones share a bidirectional relationship: hormones affect sleep quality, and poor sleep wrecks hormone production.
Estrogen – The Sleep Protector (And Disruptor)
Estrogen is often called the “female hormone,” but men produce it too (just in smaller amounts). In the context of sleep, estrogen is neuroprotective. It helps the brain utilize serotonin, the precursor to melatonin (the sleep hormone).
How Estrogen Promotes Deep Sleep
When estrogen levels are optimal, you experience:
- Shorter REM latency: You enter dream sleep more efficiently.
- Increased serotonin production: This reduces anxiety and promotes non-REM (deep) sleep.
- Lower body temperature: Estrogen helps dilate blood vessels near the skin to release heat, a critical step for falling asleep.

The Estrogen-Drop Insomnia
When estrogen plummets (during perimenopause, menopause, or postpartum), the body loses these protective effects. This leads to the hallmark “menopausal insomnia”—not just trouble falling asleep, but staying asleep.
Real-Life Example: Sarah, 49, used to sleep like a log. Suddenly, she wakes up drenched in sweat at 2 AM. Her sheets are soaked, she is shivering, and she cannot go back to sleep. This is a classic estrogen-drop hot flash triggering a nocturnal arousal.

The Hot Flash Mechanism
Estrogen withdrawal narrows the thermoneutral zone (the range where you don’t need to sweat or shiver). A tiny 0.5°F internal rise tricks the brain into thinking you are overheating. The body flips into “cool down” mode—dilating blood vessels and sweating—ripping you out of deep sleep.
Estrogen and Restless Leg Syndrome (RLS)
Low estrogen correlates with low dopamine. Dopamine deficiency is a primary driver of Restless Leg Syndrome—that creepy-crawly urge to move your legs at night. Studies show that women with low estrogen are 3x more likely to report RLS symptoms, further fragmenting sleep.
Progesterone – Nature’s Sleeping Pill
If you have ever felt overwhelmingly sleepy in the second half of your menstrual cycle (the luteal phase), you have felt the power of progesterone. After ovulation, progesterone rises sharply.
The GABA Connection
Progesterone metabolizes into allopregnanolone, a potent neurosteroid that acts on GABA-A receptors. You can think of GABA as the brain’s “off switch.” Benzodiazepines (like Valium or Xanax) work on these same receptors. Progesterone is your body’s natural, gentle Valium.

- Anxiolytic effect: It reduces racing thoughts.
- Hypnotic effect: It physically sedates the central nervous system.
When Progesterone Backfires (PMDD)
For most people, progesterone is soothing. However, for those with Premenstrual Dysphoric Disorder (PMDD), the brain reacts paradoxically to allopregnanolone. Instead of calm, it triggers severe anxiety and insomnia. This is a genetic sensitivity, not a character flaw.
Progesterone and Sleep Apnea
Progesterone is a respiratory stimulant. This is crucial for sleep because it prevents airway collapse. During pregnancy, high progesterone increases the risk of snoring, but interestingly, it protects against obstructive sleep apnea (OSA) in premenopausal women. When progesterone drops at menopause, the risk of OSA rises significantly.
Expert Quote: “Progesterone is the unsung hero of sleep. It’s the reason why women report better sleep in the mid-luteal phase of their cycle, and the reason why sleep collapses when the ovaries stop producing it.” — Dr. Fiona Baker, Human Sleep Research Program, SRI International.
Cortisol – The Midnight Thief
Cortisol follows a diurnal rhythm. It should be highest at 8 AM (to wake you up) and lowest at midnight (to let you sleep). However, chronic stress, late-night screen time, or even a 3 AM wake-up call can invert this curve.
The Vicious Cycle of Insomnia and Cortisol
When you do not sleep well, your body perceives it as a stressor. The next day, your HPA axis goes into overdrive, pumping out excess cortisol to keep you alert. That evening, the cortisol is still high, preventing melatonin release. You cannot fall asleep. You wake up tired. The cortisol spikes again. This is the biochemical definition of burnout.
The “Cortisol Awakening Response” (CAR)
Normally, cortisol surges 30–45 minutes after waking. In chronic insomniacs, the CAR is blunted (meaning you wake up groggy) OR it peaks at 3 AM (meaning you wake up in a panic).
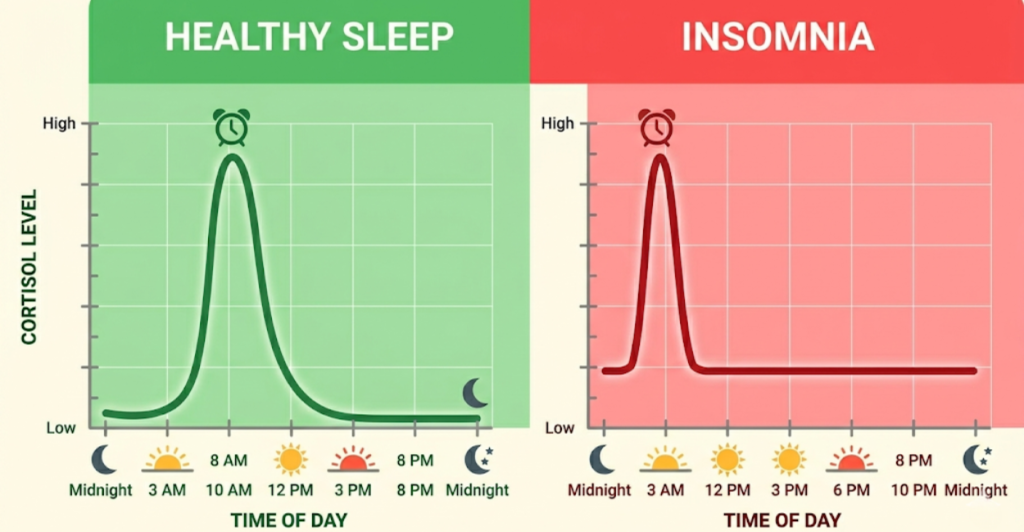
Table: Normal vs. Dysregulated Cortisol Rhythm
| Time of Day | Normal Cortisol (Healthy Sleep) | Dysregulated Cortisol (Insomnia) |
|---|---|---|
| 6:00 AM | Low (still sleeping) | High (causing early awakening) |
| 8:00 AM | Peak (Wake up energized) | Low (Wake up groggy, hungover) |
| 12:00 PM | Moderate decline | High (Anxiety, jitters) |
| 6:00 PM | Low | High (Tired but wired) |
| 10:00 PM | Trough (Ready for sleep) | Moderate (Racing mind) |
| 2:00 AM | Undetectable | Spike (The 3 AM wake-up) |
How to Lower Nighttime Cortisol Naturally
- Morning Light: 10 minutes of sunlight before 10 AM sets the HPA axis clock.
- Blood Sugar Stability: A drop in blood sugar at 3 AM triggers an adrenaline/cortisol rescue response. A small protein snack before bed (cheese, nuts) can prevent this.
- Adaptogens: Ashwagandha and Phosphatidylserine have clinical data showing a reduction in serum cortisol by up to 30% in chronically stressed adults.
The Hormonal Collision: Life Stages and Sleep Disruption
Understanding the individual hormones is one thing. Watching them battle inside a living body is another.
The Menstrual Cycle: A Weekly Shift
- Week 1 (Period): Estrogen and progesterone are low. You might sleep well but feel cold. Low progesterone can mean less deep sleep.
- Week 2 (Follicular): Estrogen rises. Sleep is generally excellent. Mood is high.
- Week 3-4 (Luteal): Progesterone rises (sleepy), then both crash (insomnia). This is when PMS insomnia hits hardest.

Perimenopause: The Rollercoaster (Ages 35-50)
Perimenopause is not a slow decline; it is a chaotic oscillation. One week you have sky-high estrogen (anxiety, palpitations), the next week zero (hot flashes, night sweats). This unpredictability makes treating sleep difficult.
Common Mistake: Using sleeping pills during perimenopause. OTC sleep aids (like diphenhydramine) often cause dry mouth and next-day grogginess. Worse, they do not address the thermoregulatory failure. You need to treat the estrogen fluctuation, not the symptom of wakefulness.
Pregnancy: The Progesterone Storm
First trimester: Progesterone skyrockets. You experience “pregnancy fatigue” and sleep 10 hours a night. Third trimester: Mechanical issues (back pain, fetal movement) plus acid reflux (caused by progesterone relaxing the esophageal sphincter) ruin sleep.
Menopause: The Estrogen Desert
Post-menopause (12 months without a period), estrogen is permanently low. Sleep architecture shifts. Women spend less time in slow-wave sleep and more time in stage 1 (light) sleep. Statistic: The National Sleep Foundation reports that 61% of postmenopausal women report insomnia symptoms, compared to 30% of premenopausal women.
H2: Myth vs. Fact: Hormonal Sleep Edition
Let’s clear up the misinformation.
Myth: “If you wake up at 3 AM, you have liver problems.”
Fact: 3 AM is the nadir (lowest point) of your body temperature and the peak time for cortisol secretion in insomniacs. It is a circadian timing issue, not an organ failure.
Myth: “Melatonin cures hormonal insomnia.”
Fact: Melatonin is a darkness signal, not a sedative. If high cortisol is the problem (the lock), melatonin is the wrong key. You need to lower cortisol first. Melatonin works best for circadian rhythm delays (jet lag), not menopausal hot flashes.
Myth: “Men don’t have hormonal sleep issues.”
Fact: Men have a daily testosterone cycle (high in AM, low at PM). Low testosterone in men is linked to increased sleep apnea and fragmented REM sleep. Additionally, aging men experience a gradual rise in cortisol and decline in growth hormone, leading to lighter sleep.
Common Mistakes People Make When Balancing Sleep Hormones
- Drinking “Nightly Wine”: Alcohol suppresses cortisol initially, but as the liver metabolizes it (around 3 AM), there is a cortisol rebound. You also lose REM sleep. Alcohol is the enemy of progesterone’s GABA effect.
- Using Screens in Bed: Blue light suppresses melatonin, but it also stimulates the HPA axis. TikTok at 11 PM tells your brain it is noon.
- Intense Evening Workouts: HIIT classes at 7 PM spike cortisol for 3-4 hours. You will be “tired but wired.” Stick to yoga or walking after 6 PM.
- Skipping Protein: As mentioned, nocturnal hypoglycemia is a major, undiagnosed cause of the 3 AM wake-up.
Practical Strategies to Rebalance Estrogen, Progesterone & Cortisol
You have the knowledge. Here is the action plan. Remember: Consult your doctor before starting supplements or HRT.
Lifestyle Interventions (The Foundation)
- Morning Sunlight (5-30 minutes): Resets cortisol rhythm. No sunglasses.
- Eat Dinner Early: Finish eating by 7 PM. Digestion generates heat (thermogenesis), which can trigger night sweats in low-estrogen states.
- Cool Your Bedroom: 65-68°F (18-20°C). If you have hot flashes, use a ChiliPad or a cooling mattress topper.
- Vagal Tone: Deep, slow breathing (4 seconds in, 6 seconds out) for 5 minutes before bed lowers cortisol via the vagus nerve.

Dietary Support
- For Low Estrogen: Phytoestrogens (flax seeds, soy, tofu) can weakly bind to estrogen receptors and reduce hot flashes.
- For Progesterone support: Vitamin B6 and Magnesium Glycinate are cofactors for progesterone production and GABA synthesis. Statistic: A 2012 study in the Journal of Research in Medical Sciences found that magnesium supplementation improved the Insomnia Severity Index score in elderly subjects by nearly 50%.
- For Cortisol control: Avoid Vitamin C deficiency. Adrenal glands have the highest concentration of Vitamin C in the body; it is required to make cortisol.
When to See a Doctor (Clinical Interventions)
- Hormone Replacement Therapy (HRT): For moderate-to-severe menopausal insomnia, micronized progesterone (Prometrium) is FDA-approved for sleep. Estrogen patches help with hot flashes. Warning: Do not use “bioidentical” creams sold online without a prescription; they are unregulated.
- SSRIs (Antidepressants): Low-dose paroxetine or escitalopram can treat both the hot flash and the associated insomnia, though they may suppress REM sleep initially.
- CBT-I (Cognitive Behavioral Therapy for Insomnia): This is the gold standard non-drug treatment. It specifically targets the “racing mind at 3 AM” by re-associating the bed with sleep, not stress.
Risk Factors & Who Should Avoid Certain Treatments
- Who should avoid HRT: Women with a history of breast cancer, blood clots, or liver disease. (Estrogen can feed certain tumors).
- Who should avoid Magnesium Glycinate: People with kidney failure (cannot excrete excess magnesium) or those on certain antibiotics (magnesium binds to them).
- Emergency Warning: If your sleep disruption is accompanied by heart palpitations, resting chest pain, or sudden severe headache, seek immediate medical attention. These can be signs of a thyroid storm or cardiovascular issue, not just hormones.
Frequently Asked Questions (FAQ)
1. Can low progesterone alone cause insomnia?
Yes. Without sufficient progesterone, the GABA receptors in your brain remain under-stimulated. This leads to “hyperarousal”—you feel tired but your brain is running a marathon. Supplementing with oral micronized progesterone is often highly effective for this specific type of anxiety-driven insomnia.
2. Does cortisol cause weight gain or sleep loss first?
Chronically high cortisol usually causes sleep loss first (the 3 AM wake-up), which then leads to cravings for sugar and fat the next day (cortisol increases insulin resistance). This visceral fat gain then worsens sleep apnea, creating a deadly loop.
3. How long does it take to fix hormonal sleep issues?
- Cortisol hygiene: 3-5 days of consistent morning light and no late eating.
- Progesterone supplementation: Effects are often felt on the first night (sedation).
- Estrogen replacement: May take 4-6 weeks to stop hot flashes fully.
4. Is it safe to take melatonin with HRT?
Generally yes, but melatonin is a hormone itself. Start low (0.5mg or 1mg). High doses (5mg+) can actually cause grogginess and weird dreams. It does not interact negatively with estrogen or progesterone.
5. Do birth control pills help with sleep?
For some, yes. Synthetic estrogen/progestin in the pill stabilizes the roller coaster cycle, which can help those with PMDD-related insomnia. For others, synthetic progestin (like levonorgestrel) is androgenic and can actually cause anxiety and worsen sleep. It varies by individual.
Conclusion: Listening to the Language of Your Body
You are not losing your mind because you are lying awake at dawn. You are losing your hormonal balance. The interplay between estrogen, progesterone, and cortisol is delicate, ancient, and powerful. When these three are in sync, sleep feels effortless. When they clash, it feels like a war inside your chest.
The good news is that unlike many medical mysteries, hormonal sleep disruption is highly treatable. By tracking your cycle (or lack thereof), adjusting your light exposure, managing your blood sugar, and having an honest conversation with your doctor about HRT or supplements, you can reclaim the night.
Tonight, don’t fight the 3 AM wake-up. Observe it. Ask yourself: Am I hot? Am I racing? Did I eat sugar at dinner? The answer is a clue. And those clues will lead you back to rest.
Did this article help you identify your sleep pattern? Share it with a friend who complains about “menopausal insomnia” or “pregnancy fatigue.” And always, consult your doctor before starting a new hormone regimen.
Medical Disclaimer
The information in this article is for educational purposes only and is not a substitute for professional medical advice. Hormonal imbalances can indicate serious underlying conditions. Always consult a qualified healthcare provider before starting any new supplement, diet, or treatment plan.
References & Trusted Sources
- The North American Menopause Society (NAMS). “Sleep and Menopause.”
- National Institute of Health (NIH): “The role of estrogen in sleep deprivation.”
- Baker, F. C., & Driver, H. S. (2007). “Circadian rhythms, sleep, and the menstrual cycle.” Sleep Medicine.
- Abbott, S. M., & Vitek, W. (2018). “Hormones and sleep.” Current Opinion in Endocrine and Metabolic Research.